







- Health and hygiene, schools and other non-household settings
- Health issues and connections with sanitation
- Research on health benefits with improved sanitation
- No evidence that this sanitation programme in rural Odisha prevented diarrhoea, soil-transmitted helminth infection, or child malnutrition (study led by Emory University)
No evidence that this sanitation programme in rural Odisha prevented diarrhoea, soil-transmitted helminth infection, or child malnutrition (study led by Emory University)
25.6k views
- joeturner
-
 Topic AuthorLess
Topic AuthorLess- Posts: 717
- Karma: 23
- Likes received: 185
Re: No evidence that this sanitation programme in rural Odisha prevented diarrhoea, soil-transmitted helminth infection, or child malnutrition (study led by Emory University)
I'm not sure this is saying much that the other report didn't say, but it is quite shocking that the presence of latrines has no particular effect on the diarrhea and helminth infection - even when latrines coverage changed from 9 to 63% of households.
With that big an engineering intervention, one would have expected some measurable change.

Please Log in to join the conversation.
You need to login to reply- Elisabeth
-
- User is blocked
- Freelance consultant since 2012
Less- Posts: 3372
- Karma: 54
- Likes received: 932
Re: New Lancet study concludes no assumed improvement from TSC (Total Sanitation Campaign, in Odisha, India)
This has been an interesting thread which is closely related to another thread called:
"The elusive effect of water and sanitation on the global burden of disease":
forum.susana.org/forum/categories/26-hea...al-burden-of-disease
(one could even think about merging the two threads but maybe it's better to keep this one separate as it started off with a very specific piece of research in Orissa - I have adjusted the thread title to make it clear what the starting point of the thread was)
I was brought back to this thread today by seeing another publication coming out from the same research team:
www.3ieimpact.org/evidence/policy-briefs...evidence-from-india/
Does building more toilets stop the spread of disease? Impact evidence from India
A 3ie-funded impact evaluation research team used a cluster-randomised controlled trial to evaluate the government’s Total Sanitation Campaign in Odisha, India to see if latrine coverage did indeed reduce exposure to disease. The intervention mobilised households in villages characterised by high levels of open defecation to build and use latrines. The study was conducted between May 2010 and December 2013, involving more than 50,000 individuals in 100 villages.
Key policy messages
The study results show that the assumption that more latrines will reduce exposure to faecal pathogens, and therefore disease, does not necessarily hold true.
During the study period, latrine coverage in the intervention villages increased from 9 per cent of households to 63 per cent, compared to an increase from 8 per cent to 12 per cent in the control villages.
The increase in latrine coverage did not prevent diarrhoea or reduce soil-transmitted helminth infection in the intervention villages. The seven-day prevalence of reported diarrhoea in children younger than 5 years was 8.8 percent in the intervention group and 9.1 percent in the control group.
This research was also co-funded by the Bill & Melinda Gates Foundation and you find it here in our project database together with some links:
www.susana.org/en/resources/projects?sea...+improved+sanitation
One of the links takes you to the SuSanA library entry for this project:
www.susana.org/en/resources/library/details/2235
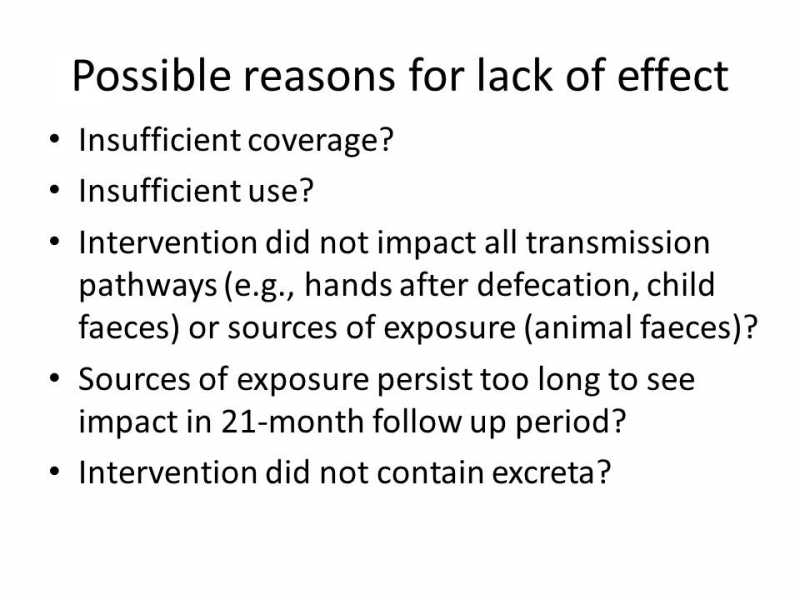
Here you find a presentation from January which I find useful and easy to read:
Please log in or register to see it.
Two very important slides towards the end:
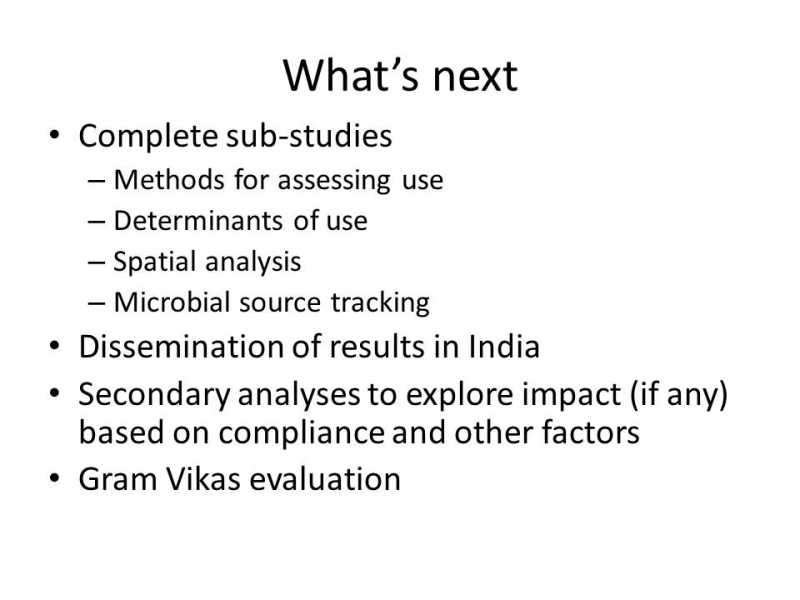
As the Gates grant still goes until 2017 (and perhaps they have more funding from other sources, too), it will be very interesting to see what else is discovered there. Wondering what is meant with "Gram Vikas evaluation"? Gram Vikas is explained here: en.wikipedia.org/wiki/Gram_Vikas **
In a way, it is (in hindsight) not really so surprising that just building toilets alone (even if they are used consistently, which they may not), is insufficient to have much of an impact on health indicators.* I guess it should always be coupled with other hygiene measures (e.g. handwashing, dealing with animal faeces in the sourroundings) as well, and probably also with mass deworming.
Kind regards,
Elisabeth
* Makes me think of Peter Harvey's question at the WEDC conference to the audience at his keynote: "Even if it was proven that having a toilet has no health benefits whatsoever, would you give up your toilet tomorrow?" - No!
** "Gram Vikas is an Indian non-governmental organization based in Orissa, and founded in 1979.[1] It uses common concerns for water and sanitation to unite and empower rural communities, including adivasi communities."
Freelance consultant on environmental and climate projects
Attachments:
-
Orissa_ppt...i_RB.jpg
(Filesize: 42KB)
-
Orissa_ppt..._RB2.jpg
(Filesize: 33KB)
Please Log in to join the conversation.
You need to login to replyRe: New Lancet study concludes no assumed improvement from TSC (Total Sanitation Campaign, in Odisha, India)
Incidence and prevalence:
Incidence is “the number of new cases per population at risk in a given time period” (please see Wiki page on incidence ). Prevalence is the “proportion of population found to have a condition ... arrived at by comparing the number of people found to have the condition with the total number of people studied, and is usually expressed as a fraction, as a percentage or as the number of cases per 10,000 or 100,000 people” (please see Wiki page on prevalence ).
In other words, prevalence measures the number of children with diarrhoea at a given point of time while incidence measures the number of children who had diarrhoea during a given time period. Since the study talks of incidence, it is “during a given time period” and not “at any point of time”. I was unable to find more details about this report, and so cannot say over what time period this statistic refers to (during a period of one year or six months, etc.,).
When we will reach “dramatic improvement”:
With regard to “dramatic improvement”, I was writing more from the perspective of cost-effectiveness. Think of the technology adoption lifecycle (TALC) and see when the 30%, 95% and 100% coverage is reached.
30% is reached after the innovators, early adopters and half of the early majority have shifted to indoor sanitation. They are the easiest to reach (compared to other categories) and yet, the diarrhoea incidence rate is around 40%. We should also note that with half of the country's population already having toilets, after taking into account the disparities in sanitation uptake between communities (for instance, villages close to major towns and cities are likely to have larger proportion of households with toilets compared to villages in remote areas and its households scoring low on development indicators), it is likely that, broadly, the innovators and early adopters already have toilets within the existing setup (ie., with thinking that toilets are costly, ability to ensure O&M given that sanitation-related activities are taboo, etc.,).
Therefore, with the same KAP-technology framework*, we would have much higher incremental cost of reaching 95% of the population (which includes till most of long-tail category have taken to indoor sanitation) and yet, 25% of the children would still have diarrhoea episodes.
* KAP - Knowledge, Attitude and Practices, all of which have been found to be critical determinants of sanitation uptake in India and elsewhere.
What is “dramatic”?
Does reduction from 40% to 25% seem dramatic? Yes, it seems dramatic but only if we do not consider the incremental cost (financial resources, time and effort) of getting to 25%. Additionally, from a programme objective & targets point of view, is 25% acceptable? Diarrhoea is a child killer by itself and also results in secondary / long-term consequences (the most discussed consequence being stunting / malnutrition). Reaching 25% means reaching most of the long-tail category and it takes the last 5% (of the same long-tail category most of which should have been already reached) to bring diarrhoeal incidence down to less than 10%. If we can reach out to most of the long-tail category, probably the last 5% will shift in an accelerated manner because of herding effect. We do not have scientific evidence for how the last 5% will behave with respect to toilets, so why leave them out of programme targets? Why give up by not even planning to achieve the goal?
So, yes, I would say that we should aim at 100% ODF communities.
Warm regards,
Sowmya
Director
Verity SmartLife Solutions
www.veritysmartlife.com
Please Log in to join the conversation.
You need to login to reply- joeturner
-
Topic AuthorLess
- Posts: 717
- Karma: 23
- Likes received: 185
Re: New Lancet study concludes no assumed improvement from TSC (Total Sanitation Campaign, in Odisha, India)
I woud assume most people would think that was a dramatic health improvement. Are you saying it is not?
Finally, clearly 100% OD free villages have to be totally free 100% of the time. The problem to me appears to be that a small number of people who are still practicing unsafe sanitation adversely affect the health outcomes for everyone. Hence I think i would say that 95% OD free - perhaps even 99% - is not good enough. Have I understood your point correctly?
Please Log in to join the conversation.
You need to login to replyRe: New Lancet study concludes no assumed improvement from TSC (Total Sanitation Campaign, in Odisha, India)
Please find below excerpt from page 37 (Box 3) of the ' Nirmal Bharat: Rural sanitation and hygiene policy 2012-2022 ' policy document:David, the issue that the study is trying to address is whether having latrines has an effect on health outcomes. I can see that education can dramatically increase the use of the latrines, do you have figures which show that 95% use is enough to dramatically improve the health outcomes?
There is little option but to aim for 100% ODF communities.A Rapid Assessment undertaken in Himachal Pradesh in 2005 revealed that in villages with ~30 per cent household toilet use, the incidence of diarrhea was reported as being around 40 per cent. Even in villages with 95 per cent household toilets, still reported around 25 per cent diarrheal incidence. Only open defecation free villages with 100 per cent usage have reported significant drop in diarrhea to less than 10%. In effect, even if a few individual households switch to using toilets, the overall risk of bacteriological contamination and incidence of disease continues to be high." The source is 'formative research by WSP - Knowledge Links for IEC Manual in Himachal Pradesh, 2005'.
Warm regards,
Sowmya
Director
Verity SmartLife Solutions
www.veritysmartlife.com
Please Log in to join the conversation.
You need to login to replyRe: New Lancet study concludes no assumed improvement from TSC (Total Sanitation Campaign, in Odisha, India)
Generating correct and adequate scientific evidence:
Let’s look at possible religious beliefs-open defecation linkages from the perspective of generating scientific evidence. Statistical analysis of MIS-type data (such as the study by Spears) can bring out the inequalities in outcome (viz., development benefits that we aim for) based on some parameter (socio-cultural, economic, gender, other). In this case, a difference in outcomes was found between Hindu and Muslim population. However, it would be incorrect to immediately conclude that religious belief must the primary cause. While a religious belief could be a cause, it need not necessarily be so – and must be backed by valid and adequate scientific evidence before drawing a conclusion. This is particularly important because interventions are designed to pivot on “key causes” and incorrect identification of “key causes” can result in ineffective outcomes.
Therefore, we must address this question: what constitutes scientific evidence to support a hypothesis that a religious belief (Hindu or other religion) is currently affecting toilet-use amongst the target population?
- This question (though relevant for sanitation from intervention design and implementation perspective) comes under the discipline of cultural anthropology. Therefore, scientific evidence must be generated through applying research methods applicable for cultural anthropology (please see Wiki page on cultural anthropology for further details). While surveys are used in cultural anthropology, it must be supported by other ethnographic and other studies.
- The evidence must be adequate to support: (a) origin of belief ie., “OD is healthy / wholesome” comes from religion and (b) the belief persists because of religion and no other reason.
A suggestion: The body of religious beliefs in India is comprised of the formal scriptures (Vedas, vedangas, Laws of Manu, etc.,) as much as mythology, legends and folklore. In other words, mythology has as much importance as scriptures in the common man’s framework of religious and ethical beliefs. For instance, more people draw their set of beliefs from the Ramayan and Mahabharata compared to the Vedas and Laws of Manu.
To understand the above, it must be remembered that, till efforts for abolishment of the caste system gained critical mass (with the efforts of Raja Ram Mohan Roy and Swami Dayananda Saraswati ), most of the scriptures were beyond the reach of the general masses. When people do not have knowledge of the scriptures, a belief can be sustained through generations, at best, as a superstition or through mythology (including legends and folklore). For instance, several gender rules in society can be sustained through mythology.
What would be interesting is if we can find legends or stories from mythology (not something obscure in layman’s knowledge – like what happened to Shvetaketu on his journey from Dwaraka to the land of the Nagas while carrying Krsna’s message would be an “obscure” story because most laypersons would not even know who is Shvetaketu) strongly upholding ‘OD is healthy / wholesome’ belief – even if it is not strong as ‘the ideal man is like Rama in the story of Ramayan’.
And, considering that quantitative studies have focused on large parts of India (whole of India / large parts of Northern India, etc.,), this myth upholding ‘OD is healthy / wholesome’ belief should be prevalent across such vast populace (instead of a legend about a deity particular to one or few contiguous villages).
A caveat here being that existence of a legend may not be a usual requirement to establish religious beliefs as the cause of current human action in anthropological studies (I have very little knowledge of anthropology) but just something I would look for given my knowledge (with all its imperfections, which should also be taken into account
 ) of India.
) of India.(b) the belief persists because of religion and no other reason: Human behaviour is influenced by several factors relating to society, including religious beliefs, cultural mores and economic priorities. To prove that OD preference is caused by religious belief, it is necessary to prove 1:1 correlation between religious beliefs and low toilet-use.
This requires a research finding that, for the same study population within the same study: (a) strongly positive association exists between OD preference and religious belief and (b) randomness / no association between OD preference and all other possible factors. In this context, we might also want to explore strength of association between religious beliefs and Knowledge-Attitude-Perceptions (KAP) interventions – for instance, do people hold on to their religious beliefs (even if it were to really exist) even after understanding the linkages between practice and health outcomes (eg., handwashing and diarrhoea).
Discussion on results from current quantitative studies:
I do not have the details of the surveys mentioned in the article, hence giving my views based on the excerpts from the article (excerpts in quotes below):
I find these sentences interesting:“A new household survey of nearly 23,000 north Indians offers more evidence, especially from Hindu households. Led by Diane Coffey, an economist at Princeton, it found that even among households with a working latrine, more than 40% reported that at least one family member preferred to defecate in the open. Those with a government-built toilet were especially likely to choose a bush instead.
In an unpublished parallel survey of Hindu-dominated villages in north India and Nepal, respondents lauded open defecation as wholesome, healthy and social. By contrast, latrines were seen as potentially impure, especially if near the home. Men often described them as for use only by women, the infirm and the elderly. In short, demand for latrines is constrained.
This suggests that the mere availability of government-built latrines will not end open defecation for decades yet. What is needed instead are public campaigns, in schools and in the media, to explain the health and economic benefits of using toilets and of better hygiene. Researchers found that only a quarter of rural householders understood that washing hands helps prevent diarrhoea.”
- “... more than 40% reported that at least one family member preferred to defecate in the open” – does this mean that some members in the same family use toilets while others prefer OD? This is possible, if we draw from the other study mentioned in the article that “Men often described them as for use only by women, the infirm and the elderly”. If this was so, how can members of the same family have different toilet-use behavior if such behavior is a result of a religious belief (and the religious belief does not make gender differences in this respect)?
- “Men often described them as for use only by women, the infirm and the elderly” – given that scriptures generally require women to maintain the highest standards of purity, is it likely that when a religious belief is the dominant reason for toilet-use behavior, women would be the ones using the toilets “especially if near the home”?
- The statement about the government-built toilets is unclear. Did choice of technology, quality of construction, etc., have any impact? Did people who had toilets connected to municipal sewer lines have the same rates of toilet-use as those with other technologies? Was the complete sanitation chain analyzed for these households as well as the ease of operating and maintaining the toilets? Further questions remain.
Warm regards,
Sowmya
Director
Verity SmartLife Solutions
www.veritysmartlife.com
Please Log in to join the conversation.
You need to login to reply- shobana
-

- WASH professional currently focussed on sanitation operator partnerships and CWIS
Less- Posts: 64
- Karma: 1
- Likes received: 28
Re: New Lancet study concludes no assumed improvement from TSC (Total Sanitation Campaign, in Odisha, India)
In my opinion, OD in India must be tackled with a multifactorial approach. I cannot see it as something associated with a Hindu tradition. Like the Attachment 1 says, the Manu law is 2000 years old and was valid during the time people had not invented toilets.
I cannot imagine villager telling that they prefer open defaecation because the Hindu -law says so. Lack of maintenance of the built toilets could be one reason. Community toilets need more awarness and education to make people understand that they have to treat the toilet as a part of their homes.
I found an interesting article in the internet explaining why India isn't able to solve this issue.
www.reuters.com/article/2014/09/03/us-ba...dUSKBN0GY1ST20140903
Sowmya here had pointed out a similar thing sometime back.
The study quotes another article, “toilets constructed or paid for by the government often remains unused or repurposed by Hindus” - this paints a starkly different picture compared to the fact only 10% do not want to use a toilet and only 2% repurposed the toilet – close to 2/3rds (41% + 22%) had poor unfinished installation or no superstructure as per a CMS 2010 Study cited in the Working Group Report on WATSAN for the XII Five Year Plan of the Government of India.
Regards,
Shobana
Programme Management Officer
UN Habitat/ GWOPA
Please Log in to join the conversation.
You need to login to reply- F H Mughal
-

- Senior Water and Sanitation Engineer
Less- Posts: 1026
- Karma: 20
- Likes received: 227

Re: New Lancet study concludes no assumed improvement from TSC (Total Sanitation Campaign, in Odisha, India)
• Access to and availability of functioning latrines, sanitation products, and services;
• Latrine product attributes (e.g., perceptions of cleanliness and durability);
• Social norms around open defecation;
• Perceived latrine affordability; and
• Competing priorities for other household expenditures.
The key attributes are: perceptions of cleanliness and, social norms around OD. In India, OD is a major problem. Review of some articles shed some light on why India continues to have OD problem.
According to the Attachment 1, “Hindu tradition, seen for example in the “Laws of Manu”, a Hindu text some 2,000 years old, encourages defecation in the open, far from home, to avoid ritual impurity. Caste division is another factor, as by tradition it was only the lowliest in society, “untouchables” (now Dalits), who cleared human waste. Many people, notably in the Hindu-dominated Gangetic plains, today still show a preference for going in the open—even if they have latrines at home.”
It further says: “A new household survey of nearly 23,000 north Indians offers more evidence, especially from Hindu households. Led by Diane Coffey, an economist at Princeton, it found that even among households with a working latrine, more than 40% reported that at least one family member preferred to defecate in the open. Those with a government-built toilet were especially likely to choose a bush instead.”
“In an unpublished parallel survey of Hindu-dominated villages in north India and Nepal, respondents lauded open defecation as wholesome, healthy and social. By contrast, latrines were seen as potentially impure, especially if near the home. Men often described them as for use only by women, the infirm and the elderly.”
The above contentions are more than clear as to why OD continues to be a problem in India. It is not a question of brick and mortar, but a drastic change in perceptions and behaviour. While Attachment 2 shows end of OD in Mali, Attachment 3 shows an approach in solving the problem, and that is the behaviour change.
F H Mughal
Karachi, Pakistan
This message has attachments files.
Please log in or register to see it.
Please Log in to join the conversation.
You need to login to reply- bracken
-

- Working throughout Africa since 1996 in development cooperation. Involved with sustainable sanitation systems since 2002. Currently working for the AHT GROUP AG (a private consultancy office in Germany).
Less- Posts: 47
- Karma: 14
- Likes received: 33
Re: New Lancet study concludes no assumed improvement from TSC (Total Sanitation Campaign, in Odisha, India)
I haven't read the study in detail yet but a brief scan does reinforce the sneaky feeling I've been having for a few years now that the mad rush to reach the numbers for 2015 won't be having the expected public health impact.
I was writing something yesterday following some time in a southern African country where CLTS has been quite aggressively established as the only show in town when it comes to improving sanitation and hygiene, and was trying to formulate this unease as follows:
"Sanitation and hygiene promotion interventions are carried out in order to reduce the impact of water and excreta related communicable diseases, and not just to increase the number of toilets in an area.
Promoting safe sanitation and hygiene is not simply about promoting access to latrines because, with a tradition of ‘open defecation’, access to a toilet does not always mean use of a toilet.
It is not only the use of a toilet, as unsanitary latrines (those that fail to confine excreta) may pose a greater health risk than ‘open defecation’.
Nor is it simply the use of a sanitary latrine, because even if individuals hygienically use and maintain a sanitary latrine, and practice hand-washing at critical times, safe sanitation and hygiene is still not assured, as the sanitary behaviour of an individual can becompromised by the unsanitary behaviour of others."
This article may help me clarify those arguments.
AHT GROUP AG
Management & Engineering
D-45128 Essen, Huyssenallee 66-68
Germany
Please Log in to join the conversation.
You need to login to reply- joeturner
-
Topic AuthorLess
- Posts: 717
- Karma: 23
- Likes received: 185
Re: New Lancet study concludes no assumed improvement from TSC (Total Sanitation Campaign, in Odisha, India)
Please Log in to join the conversation.
You need to login to replyRe: New Lancet study concludes no assumed improvement from TSC (Total Sanitation Campaign, in Odisha, India)
UN Water came out with a stat that 44 million pregnant women worldwide will contract intestinal worms this year because of OD. That means the foetus will be deprived of nutrients and disadvantaged before he or she is even born. It isn't rocket science that children will suffer. No toilets mean poor health and prolonged illness, and a lack of money to rebuild fragile bodies. Of course they will be stunted. Stunted in more ways than just body growth or brain development, tragically stunted in opportunity and the chance to fulfil potential.
Please Log in to join the conversation.
You need to login to replyRe: New Lancet study concludes no assumed improvement from TSC (Total Sanitation Campaign, in Odisha, India)
It's time again to take a longer look at top-down subsidies. See Krischan's June post on smart subsidies.
forum.susana.org/forum/categories/142-up...ation-subsidies#9033
And for a rather good overview on subsidies go to the Seecon SSWM toolbox
www.sswm.info/category/step-university/m...water-supply/furt-71
Stockholm Environment Institute
This email address is being protected from spambots. You need JavaScript enabled to view it.
www.sei.org
www.ecosanres.org
Please Log in to join the conversation.
You need to login to reply- Health and hygiene, schools and other non-household settings
- Health issues and connections with sanitation
- Research on health benefits with improved sanitation
- No evidence that this sanitation programme in rural Odisha prevented diarrhoea, soil-transmitted helminth infection, or child malnutrition (study led by Emory University)